Sliding Scale Insulin
What is sliding scale insulin (SSI)?
- SSI is a method used to manage blood glucose levels by adjusting the insulin dose based on the patient’s current blood glucose level
- It is frequently seen in place of prandial insulin in the outpatient setting - when combined with basal insulin, this is referred to as a “sliding scale-basal insulin” regimen
Pros & Cons of SSI
Pros:
- Easily adjustable
- Can be personalized for each patient
Cons:
- Sliding Scale insulin is based on pre-meal glucose levels with no regard to post-meal spike
- Rather than preventing hyperglycemia, it is more of a reactive way of treating high glucose after it has occurred – referred to as a “correction” dose
- Can cause wide fluctuations in blood glucose, creating a potentially harmful “rollercoaster” effect
- Increased risk of “insulin stacking”, as the duration of action with insulin varies
- When used alone, patients on only SSI could have a suboptimal TDD of insulin
- Only safe and effective if used with consistent diet, meal times, and exercise (little room for variation)
- Risks seen with surgical procedures as recovery and resolution to certain health conditions is negatively impacted by the “rollercoaster” patterns seen with SSI
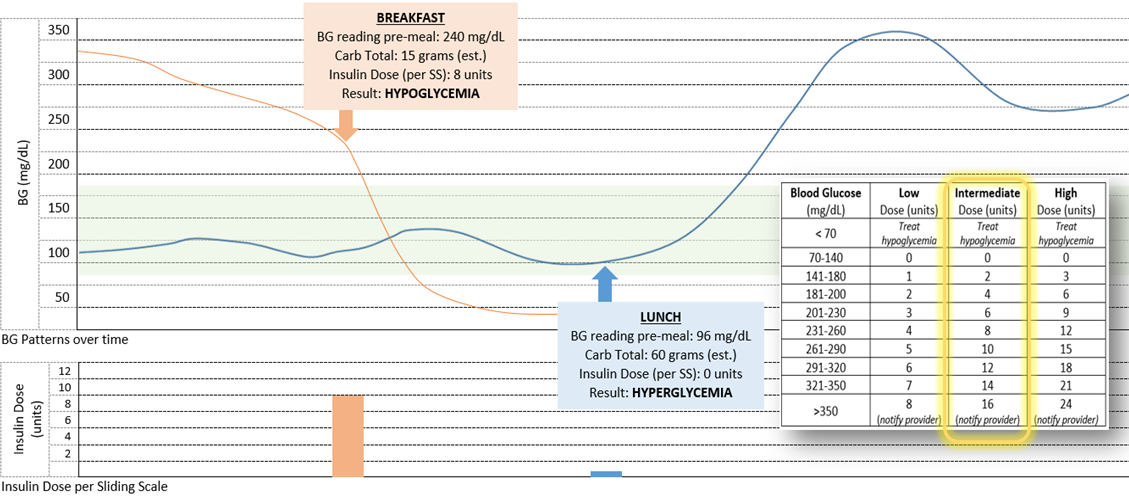
ISSUE: True sliding scale is based on blood glucose levels and designed to be used as a “correction dose”. It is possible to factor in meal/carb intake, but prescribers frequently give patients SSI “charts” or regimens based on BG alone.
Example: mismatched insulin doses with BG patterns and insulin needs when SSI is used as prandial coverage and based solely on the pre-meal BG reading
Guideline Recommendations on Sliding Scale Use (varying sources):
- Hospitalized patients with diabetes and adequate nutritional intake should be on basal/bolus scheduled doses with an additional correctional scale (sliding scale) only used if needed (ADA)
- Prolonged and/or exclusive use of SSI alone is strongly discouraged inpatient, except for diabetic patients with mild hyperglycemia (glucose in target range most of the time) and mild or occasional hyperglycemia
- SSI is not to be used as long-term diabetes treatment in long term health facilities (Choosing Wisely Campaign)
ADA Guideline Recommendations on Adding & Using Insulin
- Strong Recommendation: Consider GLP-1 RA or GIP/GLP-1 RA before initiation of any insulin
- If GLP-1 RA / GIP/GLP-1 RA is not appropriate or already titrated to max tolerable dose:
- Add basal insulin (10 units daily or 0.1-0.2 units/kg/day)
- Titrate based on FBG: increase 2 units every 3 days to reach FBG goal
- If unprovoked hypoglycemia occurs, decrease dose by 10-20%
- If FBG is at goal but prandial BG or A1C is elevated, reevaluate GLP-1 RA or GIP/GLP1-RA before prandial insulin
- Adding prandial insulin if/when necessary:
- Initiation: one dose with the largest meal or the meal with largest post-prandial elevation
- 4 units/day or 10% of basal dose
- If A1C < 8%, consider lowering basal dose by 4 units or 10%
- Titration: increase by 1-2 units or 10-15% twice weekly to reach PPG goal
- For unprovoked hypoglycemia, decrease dose by 10-20%
- Add doses of prandial in stepwise fashion as needed, until full basal-bolus regimen is established
Have others encountered misuse of SSI? How have you navigated the situation? Does anyone have experience transitioning from SSI to something else? Please share thoughts, experiences, and recommendations!
References:
- https://pmc.ncbi.nlm.nih.gov/articles/PMC6551975/
- https://www.medicalnewstoday.com/articles/317171#who-uses-it
- https://www.aafp.org/pubs/afp/issues/2010/0501/p1130.html#evidence-against-sliding-scale-insulin
- https://www.endocrinepractice.org/article/S1530-891X(22)00576-6/fulltext
- Sliding-Scale Insulin | Diabetes Care | American Diabetes Association
- Type 2 Diabetes Mellitus: Outpatient Insulin Management | AAFP
Taylor Pennisi, PharmD, BCACP, BC-ADM
Contributing Authors: Payton Alexander, PharmD Candidate 2026; Rachel Blocker, PharmD Candidate 2025