|
On November 1, the Centers for Medicare & Medicaid Services (CMS) released the Medicare Physician Fee Schedule (MPFS) final rule. This rule updates payment rates for calendar year (CY) 2019 and addresses other Medicare policies including, improving Medicare recognition of telehealth services and updates to the Quality Payment Program (QPP). These changes will apply to services furnished under the MPFS on or after January 1, 2019.
What do I need to know?
A detailed analysis of the MPFS is provided below, but here are some of the highlights:
- Payment rates for the DSMT codes G0108 and G0109, as well as for the MNT codes 97802-97804, increased slightly from the 2018 rates.
- CMS finalized NEW Chronic Care Management Remote Physiological Codes. Learn more about how diabetes educators may use these codes.
- CMS established codes for virtual check-ins and communication technology-based services in FQHCs and RHCs
- CMS did not address barriers to DSMT or virtual MDPP.
- Though not in the MPFS final rule, CMS has also updated the CY 2019 MDPP payment rates.
Want to learn more? Register for AADE’s webinar entitled “Annual Reimbursement Update for 2019” scheduled for December 12 from 1:00-2:30pm Eastern. In addition to the topics listed above, this webinar will also discuss CMS’ proposed coding changes for Evaluation and Management services.
MPFS Final Rule Analysis
Payment Conversion Factor
The CY 2019 conversion factor is $36.0391, an increase from the 2018 conversion factor of $35.9996. The conversion factor is used to calculate the payment rate for services paid under the MPFS.
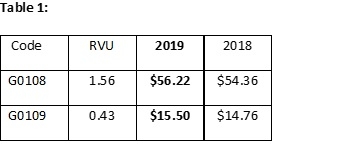
Increased Valuation for Diabetes Self-Management Training (DSMT) Codes (G0108 and G0109)
AADE was pleased to see CMS finalize a slight increase in payment rates for codes G0108 (Diabetes outpatient self-management training services, individual, 30 minutes) and G0109 (Diabetes outpatient self-management training services, group session (2 or more patients), per 30 minutes). See Table 1 for payment rates.
Chronic Care Remote Physiological Monitoring (CPT codes 99453, 99454, and 99457)
In 2017, AADE and other stakeholders worked with the American Medical Association (AMA) Relative Value Scale Update Committee (RUC) to survey and revalue these codes. Based on this review, the AMA RUC submitted valuation recommendations to CMS, which included a recommended reduction to the practice expense values for these codes. In the MPFS proposed rule, CMS did not accept the AMA RUC proposed reductions in the practice expense for these codes, thus preserving the value of these codes This action reflects ongoing advocacy and outreach to CMS by AADE on behalf of its members.
In the CY 2018 MPFS final rule, CMS unbundled and finalized separate payment for CPT code 99091. This code is defined as the “collection and interpretation of physiologic data (eg, ECG, blood pressure, glucose monitoring) digitally stored and/or transmitted by the patient and/or caregiver to the physician or other qualified healthcare professional, qualified by education, training, licensure/regulation (when applicable) requiring a minimum of 30 minutes of time.” Though providers were pleased to see a new separate payment for CPT code 99091, many recognized that this code did not accurately reflect how current remote physiological monitoring (RPM) services are delivered. To address this, the AMA CPT Editorial Panel revised one code and created three new codes to describe RPM and management. CMS finalized the three new codes to take effect on January 1, 2019. A description of those codes is below:
CPT code 99453: Remote monitoring of physiologic parameter(s) (eg, weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment.
CPT code 99454: Remote monitoring of physiologic parameter(s) (eg, weight, bloodpressure, pulse oximetry, respiratory flow rate), initial; device(s) supply with daily recording(s) or programmed alert(s) transmission, each 30 days.
CPT code 99457: Remote physiologic monitoring treatment management services, 20 minutes or more of clinical staff/physician/other qualified healthcare professional time in a calendar month requiring interactive communication with the patient/caregiver during the month.
Considerations for Diabetes Educators
Of note for diabetes educators is who can perform these services. The original RPM code, CPT code 99091, was restricted to “physicians and other qualified healthcare professionals…” One of the new codes, CPT code 99457, allows RPM services to be performed by the physician, qualified healthcare professional, or clinical staff. Clinical staff includes providers like RNs and medical assistants, though this is subject to state law scope of practice and state law supervision requirements. CMS notes in the final rule that all practitioners must practice in accordance with applicable state law and scope of practice laws. The term “other qualified healthcare professionals” used in CPT 99457 is a defined term, and that definition can be found in the CPT Codebook.
CMS also stated that CPT code 99457 describes professional time and “therefore cannot be furnished by auxiliary personnel incident to a practitioner’s professional services.” Providers must adhere to direct supervision requirements, though many are asking CMS to change their position on this to allow for general supervision, which is more in line with the Chronic Care Management (CCM) codes.
Expect More Guidance from CMS
CMS received many questions related to use of these codes during the MPFS proposed rule comment period. In the final rule, CMS announced that they would issue additional guidance to help further inform providers on how to utilize these codes.
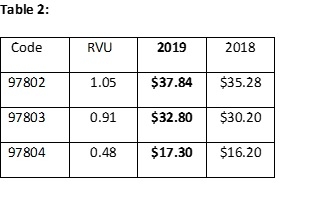
Other Codes of Interest: Medical Nutrition Therapy Procedure Codes
CMS finalized the CY 2019 payment amounts for CPT codes 97802-97804. These codes also saw a slight payment increase from 2018. See Table 2 for the estimated values of each code.
Recognizing Communication Technology-Based and Remote Evaluation Services for Rural Health Clinics (RHCs) and Federally Qualified Health Centers (FQHCs)
CMS finalized how RHCs and FQHCs bill for communication technology-based services and remote evaluation services that are furnished by an RHC or FQHC practitioner when there is no associated billable visit. This includes what is referred to as “Brief Communication Technology-based Service” for a “virtual check-in” and a remote evaluation of recorded video and/or images. The virtual check-in visit would be billable when a physician or nonphysician practitioner has a brief, non-face-to-face check-in with communication technology to assess whether a patient’s condition necessitates an office visit. This virtual check-in cannot be related to an E/M service provided in the previous 7 days or result in a service or procedure in the next 24 hours or soonest available appointment. RHCs and FQHCs will be able to bill for these services using the newly created RHC/FQHC Virtual Communication Service HCPCS code G0071. This payment will be set at the average of the MPFS national non-facility payment rates for communication technology-based services and remote evaluation services.
AADE did seek clarification from CMS to determine if these services can be used by physicians or other nonphysician practitioners to assess whether DSMT is needed. CMS states that communication technology-based and remote evaluation services would be billable by RHCs and FQHCs only when the discussion requires the skill level of the RHC or FQHC practitioner. If the discussion could be conducted by a nurse, health educator, or other clinical personnel, it would not be billable as a virtual communication service. CMS clarified that payment for DSMT in FQHCs would not be impacted by the new virtual communication codes.
As background, RHC and FQHC visits are in-person encounters between a patient and an RHC or FQHC practitioner furnishing a qualifying service. Of note, not all covered Medicare services qualify as an RHC or FQHC service. A DSMT service or a Medical Nutrition Therapy (MNT) service furnished by a certified DSMT or MNT provider qualifies as an FQHC visit.
The RHC and FQHC payment models are distinct from the MPFS payment model in that RHC and FQHC payment rates reflect the cost of all services and supplies that an RHC or FQHC furnishes to a patient in a single day. Currently, if a service is provided via a communication-based technology and it results in a face-to-face billable visit, that service would be considered part of the RHC or FQHC visit and is not separately billable. If the service did not result in an in-person visit, there would be no payment for the service. This new CMS policy serves to address this by reimbursing RHCs/FQHCs for virtual check-ins that do not result in a billable visit.
Modernizing Medicare Physician Payment by Recognizing Communication Technology-Based Services
CMS finalized proposals to pay separately for two newly defined physicians’ services furnished using communication technology:
- Brief communication technology-based service, e.g. virtual check-in (HCPCS code G2012) and
- Remote evaluation of recorded video and/or images submitted by an established patient (HCPCS code G2010)
Practitioners could be separately paid for the brief communication technology-based service when a patient checks in with the practitioner via telephone or other telecommunications device to decide whether an office visit or other service is needed. This would increase efficiency for practitioners and convenience for beneficiaries. Similarly, the service of remote evaluation of recorded video and/or images submitted by an established patient would allow practitioners to be separately paid for reviewing patient-transmitted photo or video information conducted via pre-recorded “store and forward” video or image technology to assess whether a visit is needed.
CMS is also finalizing policies to pay separately for new coding describing chronic care remote physiologic monitoring (CPT codes 99453, 99454, and 99457) and interprofessional internet consultation (CPT codes 99451, 99452, 99446, 99447, 99448, and 99449).
Quality Payment Program Future Reporting Considerations: Public Health Priority Sets
CMS used the MPFS proposed rule to seek feedback on their proposal to engage in future rulemaking to develop Merit-based Incentive Payment System (MIPS) public health priority sets across all four performance categories (quality, improvement activities, Promoting Interoperability, and cost). AADE offered comments on this proposal, suggesting potential priority sets for diabetes. In the final rule, CMS indicated that they will take these comments into consideration as they develop future policy proposals.
Addressing Barriers to DSMT
In AADE’s MPFS proposed rule comments to CMS, we expressed our disappointment that the agency did not address barriers to DSMT. The Diabetes Advocacy Alliance (DAA) also offered similar comments to CMS. CMS acknowledged these comments and stated that they would consider these issues for future rulemaking. AADE will continue to advocate before CMS to reduce the barriers that Medicare beneficiaries with diabetes face in accessing DSMT.
Virtual Medicare Diabetes Prevention Program (MDPP)
In our MPFS proposed rule comments, AADE indicated that we had hoped CMS would establish a virtual MDPP pilot in the proposed rule. CMS did not specifically address these comments in the final rule. AADE will continue to look for opportunities in future rulemaking.
Other Reimbursement Updates
Updated Calendar Year (CY) 2019 Medicare Diabetes Prevention Program (MDPP) Payment Rates
Though not specifically addressed in the MPFS final rule, CMS did update the MDPP payment rates for 2019. Click here for more information.
Learn More!
Click here for more information on the MPFS final rule, including a helpful fact sheet and other relevant information. Also, here is a link to AADE’s comments in response to the MPFS proposed rule released in July. CMS addressed many of the policy points raised by AADE in the MPFS final rule.
Don’t forget to register for AADE’s webinar entitled “Annual Reimbursement Update for 2019” scheduled for December 12 from 1:00-2:30pm Eastern!
Subscribe to the Advocacy Forum
Interested in receiving more advocacy updates like the ones included above? Subscribe to the Advocacy Forum on My AADE Network.
|