We will see much in the news this month about cardiovascular disease and our risk for it. I am glad to have the awareness. Please consider my thoughts about the origins of risk and ask yourself: what is your role here? One of the many things I love about the Association of Diabetes Care & Education Specialists is that we are multidisciplinary. Each part of the body important, each has a role and a function. Thank you for your engagement and tenacity to pursue this important work.
I am passionately concerned for the welfare of our children with all diabetes, but especially type 2 diabetes. The CDC Diabetes in Youth Report shows that members of racial and ethnic minority groups had the highest rates of new cases. See the chart below.
Figure 6. Incidence of Type 2 Diabetes Among U.S. Children and Adolescents Aged 10 to 19 Years, by Race/Ethnicity, 2011-2012

Note: American Indian youth who participated in the SEARCH study are not representative of all American Indian youth in the United States. Thus, these rates cannot be generalized to all American Indian youth nationwide.
Data source: SEARCH for Diabetes in Youth Study.
Personally, three of our four children have type 1 diabetes with no family history. Interestingly, I became an RN and then a CDE seven years before the first child was diagnosed, as people always ask! I am so thankful for their general health, but am drawn to the startling statistics of accelerated risk of medical complications for children and adolescents with type 1 and type 2 diabetes. These statistics draw me in because I strongly believe that each of us can change the risk and outcomes of the children affected by prediabetes and diabetes.
My day job is the Inpatient Diabetes Care Coordinator of a 300+ bed teaching hospital in Southeast Pennsylvania. I had my first 28 year old patient (white, non-Hispanic) with newly diagnosed diabetes, A1C > 11%, and a Myocardial Infarction at our hospital. He required two stents and insulin to be safely discharged. Unbelievable. I thought it was a unique situation but just in the last month we had a person with type 1 diabetes in the ED with chest pain, a clot in the left anterior descending (LAD) coronary artery requiring stent placement! He was 21 years old (black, non-Hispanic) with an A1C > 11% and a duration of diabetes greater than 15 years. I had a consult for a complex care patient seen in our cardiology outpatient area. A 32 year old (black, non-Hispanic) woman post ST elevation myocardial infarction (STEMI) and drug eluding stent to the LAD sat before me on the exam table with her two year old on her lap. Her recent A1C was 12.9% with a history of hypertension. This is startling and preventable. Something MUST BE DONE to not only raise awareness but raise resources, activate thought leaders and other actions to help our rising generation prevent diabetic complications.
I had opportunity to attend the New Jersey Hospital Association (NJHA) “Patients, Prejudice and Policy” conference with my work in complex care in April of 2019. The First Lady of New Jersey, Tammy Murphy, is dedicated to changing the landscape in New Jersey through conversations on health equity and eliminating unconscious biases. She kicked off the remarkable meeting by broadening awareness of the racial disparities in fetal and maternal mortality. It seems clear from the charts below that disparate populations continue to face such disadvantages. Look at the rates of arterial stiffness leading to hypertension and CVD! Alarming. It makes sense in a high-risk pregnancy that there remain hidden risks, like the iceberg analogy, just waiting to become manifest in cardiometabolic complications (blood clots, preeclampsia and/or death).
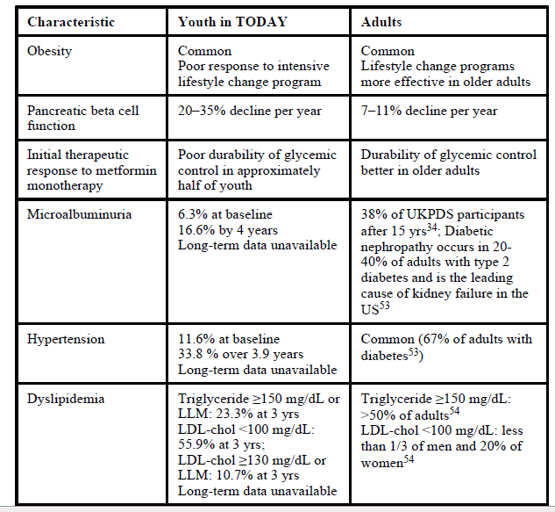
We should not allow another four years to pass – look below at the complications (Table 1) that will arise in just four years. How many more young people will enter our doors with another NSTEMI or STEMI requiring stents and life altering medications requiring adherence? Page 7 of the Youth-Onset Type 2 Diabetes: Lessons Learned from the TODAY Study, states the following:
The high incidence of atherogenic lipid profiles and worsening of cardiovascular risk factors observed during the first 36 months of the TODAY study suggest the possibility of premature onset of cardiovascular disease in the future for youth-onset type 2 diabetes. It has been estimated that children with type 2 diabetes with onset at age 10 years will lose 19 life years43. This underscores the importance of developing effective treatment strategies and interventions to lower this risk.
The evidence-based research speaks to a growing need to bring far greater awareness to this issue. The tables below reference the outcomes from the TODAY Study. Here is a link to slides from the ADA Scientific Sessions on TODAY2 (note: they ask that you enter your e-mail to access the slides). The SEARCH for Diabetes in Youth study, published February 28, 2017, in the Journal of the American Medical Association remains pivotal for me. Lastly, here is a link to the CDC Vision Health Fact Sheet which emphasizes the disparate outcomes in diabetic retinopathy.
Table 1

https://www.nih.gov/news-events/news-releases/youth-type-2-diabetes-develop-complications-more-often-type-1-peers
In honor of February as American Heart Month, I challenge us all to advocate for more public awareness regarding the connection between diabetes and cardiovascular disease. What comes to mind as your next move? Research the topic, discussions with colleagues, schools, community leaders? Please, just make a promise you won’t wait four years. Make use of our ADCES resources here.